
UCSD Musculoskeletal Radiology
bonepit.com
Patella tracking
|
|
UCSD Musculoskeletal Radiology bonepit.com Patella tracking |
The new sports medicine orhtopedic consultant; Robert Afra would like patella tilt and subluxation measured as follows:
Two new sequences for knee patella tracking study.
1. Flexion views:
Mid patella single 2.5/3mm axial view @ right angles to patella articular surface (will need to angle gantry) @ 0, 15,30,45 degrees knee flexion, toes pointing straight up. The degree of flexion can be eyeballed with experience, or a goniometer may be employed. The angle can be checked on the lateral scout. Send only bone algorithm.
The following 3 radiologist measurements are made on 30 degree angle view only.
Patella tilt: Base line is line between posterior femoral condyles. Line on lateral facet of patella. If angle between these is less than 10 degrees then abnormal.
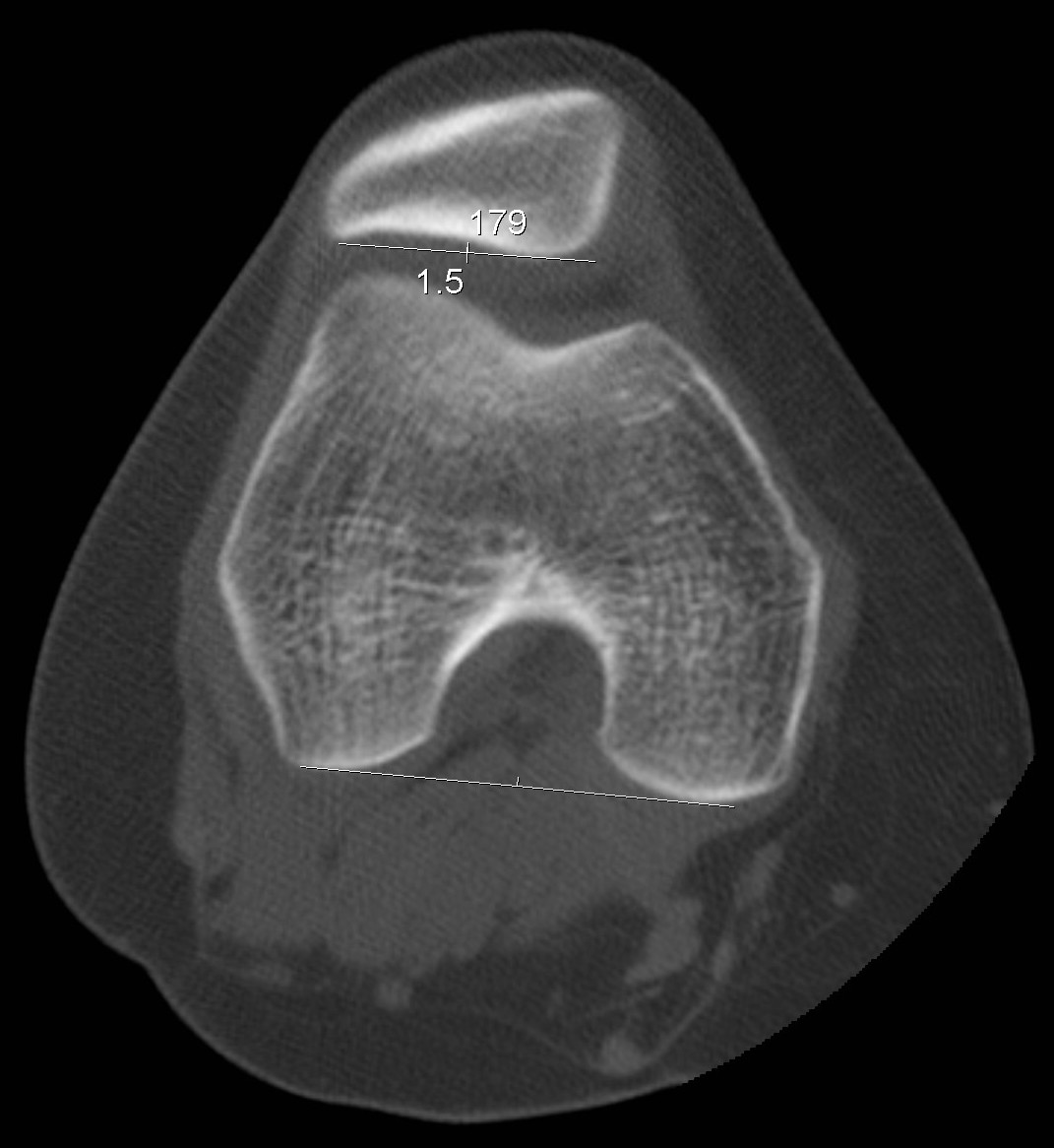
Lateral trochlear angle: Same base line. Line on lateral side of trochlear groove. Angle greater than 11 degrees is good.

Subluxation: Measured in mm. Draw lines down either side of trochlear groove. Draw bissector of this angle from its apex. Measure distance of patella apex from this line.

2. Gunsight views. Perform whilst the knee is at 30 degrees in the middle of the above series.
Toes pointing straight up. No movement between slices. Knee 30 degrees flexion. ) 0 degree angle gantry.
Axial 2.5/3mm cuts from top of trochlea notch/top of patella to bottom of tibial tubercle.
Radiologist to measure “Tibial tubercle to trochlear groove displacement”: Draw posterior femoral condyle line as above. Draw line at 90 degrees to this from apex of trochlear groove. Transpose parallel lines to tibial tuberosity. Measure distance difference of the two intersecting points along the line of the condylar line to a fixed point such as the edge of the film and subtract. In other words what is the lateral distance between these two parallel lines one from the tibial tubercle, one from the apex of the trochlea notch, both at right angles to the line between the posterior femoral condyles.


This all seems very self explanatory.
Tudor